Expert insights on vision correction, eye care, and the latest treatments from Khanna Vision Institute
.kvi-blog-fragment#kvi-blog-red-light-rlrl { --accent: #c2410c; --accent-muted: #9a3412; --accent-soft: #fff7ed; --ink: #0f172a; --muted: #47556...
Read More.kvi-blog-fragment#kvi-blog-annual-exam { --accent: #c2410c; --accent-muted: #9a3412; --accent-soft: #fff7ed; --ink: #0f172a; --muted: #475569; ...
Read MoreTECNIS PureSee vs PanOptix vs TECNIS Odyssey | Khanna Vision Institute :root{ ...
Read MoreBVI FINEVISION HP vs PanOptix vs TECNIS Odyssey | Khanna Vision Institute :root...
Read MoreSMILE vs LASIK is one of the most common questions for patients who want a painless laser vision correction and a fast recovery. SMILE is a minimally invasive, flap-free procedure that may feel gentler and often causes less dryness, while LASIK is well-known for extremely fast visual clarity soon after surgery. At Khanna Vision Institute, Dr. Rajesh Khanna uses advanced imaging and personalized evaluations to recommend the safest option based on your eyes, lifestyle, and long-term expectations.
Read More
Learn how presbyopia affects hairstylists and discover advanced treatment options. Find out how Dr. Rajesh Khanna helps Bakersfield professionals restore clear, comfortable vision.
Read MoreReLEx SMILE is a flap-free laser vision procedure that corrects myopia and astigmatism through a tiny incision, often with less dryness and fast recovery. Many patients praise quick results, comfort, and clear vision at Khanna Vision Institute.
Read MoreLASIK can feel surprisingly easy with the right surgeon—fast procedure, minimal discomfort, and clearer vision often by the next day. A consultation confirms whether LASIK or options like SMILE/EVO ICL fit your eyes.
Read MoreAffordable LASIK in Los Angeles is possible with financing and a proper candidacy exam. It’s a quick, safe procedure with fast recovery and long-term value compared to years of glasses or contacts.
Read MoreAffordable LASIK is possible with transparent pricing, flexible financing, and modern all-laser technology. A consultation confirms candidacy and helps you choose LASIK or alternatives like SMILE or EVO ICL.
Read MoreLASIK can correct astigmatism by reshaping the cornea for sharper, more stable vision. It’s quick, safe, and often reduces or removes the need for glasses or contacts after a candidacy exam.
Read MorePresbyopia is age-related near-vision blur that usually starts after 40. It’s treatable with reading glasses, contacts, monovision LASIK, or lens implants like PIE after an eye exam.
Read MorePinguecula is a common sun-related bump on the white of the eye. Eye drops and UV protection often control symptoms, but cosmetic removal is an option if irritation or appearance concerns persist.
Read MoreSMILE can remove the hassle of glasses and contacts, with a quick, flap-free procedure and fast recovery. Many professionals feel sharper focus, better comfort, and more confidence at work after SMILE.
Read MoreCataract surgery restores clear vision by replacing the cloudy natural lens with a clear IOL. With modern laser-assisted technology, most patients see brighter and sharper within days after a quick, safe procedure.
Read MoreBlephEx is a quick in-office eyelid cleaning that removes biofilm and debris causing Meibomian Gland Dysfunction (MGD). It helps restore tear quality and reduce chronic dry eye symptoms fast.
Read MoreSMILE is a flap-free laser vision procedure with a tiny incision, fast recovery, and lower dry-eye risk than LASIK. It’s ideal for active lifestyles and offers stable, long-lasting clear vision.
Read MoreBefore PIE (Presbyopic Implant in Eye), you’ll need a full eye exam and precise measurements to choose the right lens. Treat any dry eye first, then follow simple recovery steps and follow-ups for best results.
Read MoreBefore EVO ICL surgery, get a full eye exam, follow pre-op instructions, understand the lens procedure, plan a short recovery, and attend follow-ups for long-term safety and best results.
Read MoreChristmas SMILE Gift Certificate – Calabasas: Gift a SMILE Pro (flap-free laser vision correction) credit that can be used at Khanna Vision Institute (Beverly Hills / Westlake Village). Typically $3,495–$3,995 per eye, no expiry, transferable, often FSA/HSA eligible — buy now, schedule in 2026.
Read MoreChristmas SMILE Gift Certificate – Burbank: Give the gift of clear vision with SMILE Pro (flap-free laser vision correction). Certificates never expire, are transferable, and are often FSA/HSA eligible. Use at Khanna Vision Institute (Beverly Hills or Westlake Village) and schedule in 2026. SMILE typically $3,495–$3,995 per eye.
Read MoreA Beverly Hills SMILE (SMILE Pro) Christmas Gift Certificate is a premium, flap-free laser vision correction option for someone tired of glasses or dry contacts. SMILE uses a tiny keyhole incision (no corneal flap), supports active lifestyles, and is associated with fast recovery and often less dryness vs. traditional LASIK. Gift certificates never expire, are transferable, and are typically FSA/HSA eligible—purchase now and schedule the consultation/surgery in 2026 at Khanna Vision Institute’s Beverly Hills or Westlake Village locations.
Read MoreA Westlake Village EVO ICL Christmas Gift Certificate is a life-changing option for loved ones who struggle with dry contacts or strong glasses and aren’t ideal LASIK/SMILE candidates—offering clear, stable, natural-feeling vision with a reversible implant lens. Certificates never expire, are transferable and FSA/HSA eligible, and can be used toward any procedure—purchase by phone and schedule a 2026 consultation.
Read MoreA West Hollywood EVO ICL Christmas Gift Certificate is a high-impact upgrade for creatives and professionals who want clear, confident vision when LASIK/SMILE aren’t suitable—especially with high prescriptions or thin corneas. Certificates never expire, are transferable and FSA/HSA eligible, and can be used toward any procedure—purchase by phone and schedule a 2026 consultation.
Read MoreA Thousand Oaks EVO ICL Christmas Gift Certificate is a practical, family-friendly way to help someone enjoy clear, reliable vision when LASIK/SMILE aren’t ideal—especially for high prescriptions or thin corneas. Certificates never expire, are transferable and FSA/HSA eligible, and can be used toward any procedure—purchase by phone and schedule a 2026 consultation.
Read MoreA Santa Monica EVO ICL Christmas Gift Certificate is a beach-friendly vision upgrade—ideal for people who struggle with contacts, dry eyes, or high prescriptions and aren’t great LASIK/SMILE candidates. Certificates never expire, are transferable and FSA/HSA eligible, and can be applied toward any procedure—purchase by phone and schedule a 2026 consultation.
Read MoreA San Francisco EVO ICL Christmas Gift Certificate is a premium way to help someone with high prescriptions or thin corneas enjoy clear, stable vision when LASIK/SMILE aren’t ideal—great for screen-heavy, on-the-go city life. Certificates never expire, are transferable and FSA/HSA eligible, and you can purchase by phone and schedule a 2026 consultation.
Read MoreGive San Diego families a Christmas EVO ICL Gift Certificate—a meaningful option for people who aren’t ideal LASIK/SMILE candidates, offering sharp, comfortable vision (especially at night) with a reversible, FDA-approved lens. Certificates never expire, are transferable, FSA/HSA eligible, and can be applied toward any procedure—purchase by phone and schedule surgery in 2026.
Read MoreCelebrate Christmas with an EVO ICL Gift Certificate for Pasadena—a thoughtful way to help students, creatives, and professionals enjoy clearer, more comfortable vision when LASIK/SMILE aren’t suitable. Gift certificates never expire, are transferable, and can be applied to any vision correction procedure—call to purchase and schedule a 2026 consultation.
Read MoreGive someone in Pasadena a Christmas gift they’ll feel every morning: a SMILE Pro Gift Certificate from Khanna Vision Institute. It’s flap-free, gentle, and designed for active lifestyles—with many patients noticing clearer vision within 24 hours. Gift amounts: $250 / $500 (most popular) / $1,000 or custom. Never expires. Transferable. FSA/HSA eligible. Buy by phone: Beverly Hills (310) 482-1240 • Westlake Village (805) 230-2126
Read MoreGive someone in Orange County a Christmas gift that actually changes daily life: a SMILE Pro Gift Certificate from Khanna Vision Institute. It’s gentle + flap-free, built for active lifestyles, and many patients notice clearer vision within 24 hours. Gift options: $250 / $500 (most popular) / $1,000 or custom. Never expires. Transferable. FSA/HSA eligible. Buy by phone: Beverly Hills (310) 482-1240 • Westlake Village (805) 230-2126
Read MoreGive someone in Newport Beach a Christmas upgrade that lasts: a SMILE Pro Gift Certificate from Khanna Vision Institute. SMILE is gentle + flap-free, built for active lifestyles, and many patients notice clearer vision within 24 hours. Amounts: $250 / $500 (most popular) / $1,000 or custom. Never expires. Transferable. FSA/HSA eligible. Buy by phone: Beverly Hills (310) 482-1240 • Westlake Village (805) 230-2126
Read MoreGive someone in Malibu a holiday upgrade that lasts: a Christmas SMILE Pro Gift Certificate from Khanna Vision Institute. SMILE is gentle and flap-free, designed for active lifestyles, with many patients noticing clearer vision within about 24 hours. Gift certificates start at $250, can be customized, never expire, and are FSA/HSA eligible. Purchase by phone: Beverly Hills (310) 482-1240 or Westlake Village (805) 230-2126.
Read MoreGive the gift of clear vision with a Christmas SMILE Pro Gift Certificate from Khanna Vision Institute—perfect for Los Angeles residents who want freedom from glasses/contacts with a gentle, flap-free laser procedure. Certificates start at $250, never expire, and can be used toward SMILE or other vision correction. Call (310) 482-1240 (Beverly Hills) or (805) 230-2126 (Westlake Village).
Read MoreChristmas SMILE Gift Certificate – Los Angeles: Gift credit for SMILE Pro (flap-free laser vision correction) at Khanna Vision Institute (Beverly Hills / Westlake Village). Published Feb 10, 2026; typical cost $3,495–$3,995 per eye; preset gifts $250 / $500 / $1,000 + custom; no expiry, transferable, often FSA/HSA eligible.
Read MoreChristmas SMILE Gift Certificate – Laguna Beach: Gift credit for SMILE Pro (flap-free laser vision correction) at Khanna Vision Institute (Beverly Hills / Westlake Village). Published Feb 10, 2026. Typical cost $3,495–$3,995 per eye; preset gifts $250 / $500 / $1,000; custom amount option; no expiry, transferable, often FSA/HSA eligible; buy now, schedule in 2026.
Read MoreChristmas SMILE Gift Certificate – Glendale: Gift SMILE Pro (flap-free laser vision correction) credit at Khanna Vision Institute (Beverly Hills / Westlake Village). Published Feb 10, 2026. Typical cost $3,495–$3,995 per eye; preset gifts $250 / $500 / $1,000; no expiry, transferable, often FSA/HSA eligible; buy now, schedule in 2026.
Read MoreChristmas SMILE Gift Certificate – Irvine: Gift credit for SMILE Pro (flap-free laser vision correction) at Khanna Vision Institute (Beverly Hills / Westlake Village). Published Feb 10, 2026. Typical cost $3,495–$3,995 per eye; preset gifts $250 / $500 / $1,000; custom amount option; no expiry, transferable, often FSA/HSA eligible; buy now, schedule in 2026.
Read MoreChristmas SMILE Gift Certificate – Culver City: Gift SMILE Pro (flap-free laser vision correction) credit at Khanna Vision Institute (Beverly Hills / Westlake Village). Published Feb 10, 2026. Typical cost $3,495–$3,995 per eye; preset gifts $250 / $500 / $1,000; no expiry, transferable, often FSA/HSA eligible; buy now, schedule in 2026.
Read MoreSoft contact lenses are a popular, flexible way to see clearly without glasses—but long wear time, hygiene issues, and reduced oxygen flow can lead to dryness, redness, blurry vision, and eye strain. This guide explains the key pros and cons of soft lenses, common discomforts, and practical tips to stay comfortable, plus when it may be time to consider long-term alternatives like LASIK, SMILE, or EVO ICL with a personalized evaluation at Khanna Vision Institute.
Read MoreSMILE eye surgery is a flap-free laser vision correction that helps soccer players and active athletes achieve sharp, dependable vision without the hassle of glasses or the irritation of contact lenses. By reshaping the cornea through a small incision, SMILE can correct myopia and certain levels of astigmatism while often causing less dryness and offering a quick recovery—so athletes can return to training with greater comfort, confidence, and on-field focus.
Read MoreSMILE (Small Incision Lenticule Extraction) is a minimally invasive, flap-free laser vision correction performed with advanced Zeiss VisuMax technology at Khanna Vision Institute. In this patient story, Sarah—an active 29-year-old with mild dryness—chose SMILE for its tiny 2–3 mm incision, fast healing, reduced dry-eye risk, and long-term corneal stability. With personalized care from Dr. Rajesh Khanna, many patients enjoy clear vision within 24 hours and return to normal routines quickly.
Read MoreSMILE vs PRK is a common comparison for patients who want freedom from glasses and contacts but also care about comfort and recovery time. PRK removes the corneal surface layer and typically involves more irritation and a longer healing period, while SMILE is a minimally invasive, flap-free procedure that reshapes the cornea through a tiny incision—often leading to faster recovery, less dryness, and a smoother return to normal activities. At Khanna Vision Institute, Dr. Rajesh Khanna uses detailed diagnostics to recommend the safest option based on your corneas, lifestyle, and vision goals.
Read MoreSMILE surgery (Small Incision Lenticule Extraction) is a next-generation, flap-free laser vision correction that treats nearsightedness and astigmatism through a tiny 2–3 mm incision. Using advanced femtosecond laser technology such as the ZEISS VisuMax, Dr. Rajesh Khanna at Khanna Vision Institute helps patients achieve clear vision with less dryness, minimal discomfort, fast recovery, and long-term corneal stability—making SMILE an excellent option for active lifestyles and those seeking a gentle alternative to LASIK.
Read MoreSMILE eye surgery (Small Incision Lenticule Extraction) is a modern, flap-free laser vision correction that can treat myopia and certain levels of astigmatism with fast recovery and minimal discomfort. At Khanna Vision Institute, Dr. Rajesh Khanna performs a precise femtosecond-laser procedure that reshapes the cornea through a tiny incision—often leading to clearer vision within hours, less dryness than traditional methods, and a quick return to daily routines.
Read MorePterygium (“surfer’s eye”) can cause redness, irritation, and even blurred vision as it grows toward the cornea. Learn when surgery is recommended, how graft-based removal reduces recurrence, and how patients in Los Angeles find lasting relief at Khanna Vision Institute.
Read MoreMost LASIK side effects are mild and temporary—but the best results come from prevention: advanced testing, customized laser planning, and careful aftercare. Learn how Dr. Rajesh Khanna minimizes dryness, glare, and healing issues with modern all-laser LASIK at Khanna Vision Institute.
Read MorePost-LASIK life is a performance upgrade—clear, stable vision for golf, swimming, snow sports, snorkeling, and martial arts without fogging glasses or drying contacts. Discover how Khanna Vision Institute helps active patients recover fast and train with confidence.
Read MoreModern LASIK at Khanna Vision Institute is quick, gentle, and surprisingly comfortable—most patients feel only light pressure and see clearer within hours. Discover how Dr. Rajesh Khanna helps patients overcome fear and enjoy lasting, glasses-free happiness.
Read MorePRK and LASIK both reshape the cornea for clear vision, but recovery, comfort, and technique are different. Learn which option fits your corneas and lifestyle—then confirm with a personalized evaluation at Khanna Vision Institute.
Read MoreA long-time contact lens wearer shares how dryness, irritation, and constant maintenance led to a better solution—personalized vision correction at Khanna Vision Institute. Learn how SMILE, LASIK, and EVO ICL can deliver lasting freedom from contacts and clearer, healthier eyes.
Read MoreLimited-time LASIK savings at Khanna Vision Institute—premium laser technology and Dr. Rajesh Khanna’s personalized care at exceptional value. Book your consultation to see if you qualify and get clearer vision fast, often within 24 hours.
Read MoreModern LASIK at Khanna Vision Institute is designed to be gentle and predictable—most patients feel only light pressure, see clearly within hours, and experience minimal redness. Learn what happens during LASIK, how recovery feels, and who may qualify for safe, long-lasting vision correction.
Read MorePresbyopic implants (PIE) are a modern lens-replacement solution that helps adults regain clear near, intermediate, and distance vision—often reducing or eliminating the need for reading glasses. This page explains how presbyopia develops, how presbyopic intraocular lenses work, and what to expect from the quick procedure and recovery. Learn how Dr. Rajesh Khanna personalizes implant selection at Khanna Vision Institute for patients in Beverly Hills and Westlake Village.
Read MoreNew painless laser eye surgery makes vision correction safer, smoother, and more comfortable than ever—often with clear vision within hours and return to routine the next day. This article explains how modern options like All-Laser LASIK, SMILE, and EVO ICL reduce discomfort through bladeless precision, tiny incisions, and advanced eye mapping. Learn how Dr. Rajesh Khanna customizes the best procedure for your eyes and lifestyle at Khanna Vision Institute.
Read MoreModern laser eye surgery offers more precision, comfort, and choice than ever—helping many patients achieve clear vision with quick recovery and long-term stability. This article explains what “new laser eye surgery” means today, how advanced imaging creates a personalized treatment plan, and how options like SMILE and advanced custom LASIK can reduce dryness, improve corneal stability, and deliver dependable clarity. Learn who qualifies, what recovery feels like, and why patients choose Khanna Vision Institute for advanced laser vision correction with Dr. Rajesh Khanna.
Read MoreSMILE (Small Incision Lenticule Extraction) is a modern, flap-free laser procedure designed to correct myopia and astigmatism with a tiny incision and minimal surface disruption. This guide explains how SMILE reshapes the cornea from within, why many patients experience less dryness and strong long-term stability, what the procedure feels like, and what recovery typically looks like—often with clearer vision by the next day. Learn how candidacy is confirmed through a complete exam at Khanna Vision Institute with Dr. Rajesh Khanna.
Read MoreUpper blepharoplasty (upper eyelid surgery) can be performed for medical reasons—when droopy eyelid skin blocks your visual field—or for cosmetic reasons to reduce heaviness, puffiness, and sagging for a more refreshed look. This article explains the key differences, insurance considerations, what the procedure involves, typical recovery timelines, and aftercare tips, and how Dr. Rajesh Khanna may combine functional and aesthetic goals for natural results at Khanna Vision Institute.
Read MoreAll-Laser LASIK is a blade-free, modern approach to vision correction that uses two advanced lasers for greater precision, safety, and comfort. This guide explains how femtosecond and excimer laser technology creates a customized corneal flap, reshapes vision, and delivers fast recovery with minimal discomfort—often with clearer sight within 24 hours. Learn candidacy requirements, what the procedure feels like, aftercare tips, and why patients choose All-Laser LASIK at Khanna Vision Institute with Dr. Rajesh Khanna.
Read MoreA limited-time half-price LASIK offer can make world-class vision correction more affordable—but patients should still understand how LASIK works, who qualifies, and what to expect from consultation through recovery. This article explains modern bladeless LASIK technology, candidacy factors, typical comfort and healing timeline, and why a thorough exam may also reveal alternatives like SMILE or EVO ICL. Learn how pricing, financing, and long-term value are evaluated at Khanna Vision Institute with Dr. Rajesh Khanna.
Read MoreLASIK and SMILE are two leading laser vision correction options that can reduce or eliminate dependence on glasses and contact lenses. This article explains how each procedure works—LASIK with a corneal flap and SMILE with a small, flap-free incision—along with key differences in candidacy, dryness risk, recovery, and long-term comfort. Learn how detailed imaging and a personalized evaluation help patients choose the best option at Khanna Vision Institute with Dr. Rajesh Khanna.
Read MorePterygium (“surfer’s eye”) can affect corneal surface health, dryness, and vision quality—so choosing the right laser vision correction needs careful screening. This article compares LASIK vs. SMILE for patients with current or past pterygium, explaining why flap-based LASIK may require full healing after pterygium removal, while SMILE’s flap-free, small-incision approach can be a gentler option for sensitive or drier eyes. Learn how corneal mapping and tear-film testing guide safe, personalized recommendations at Khanna Vision Institute with Dr. Rajesh Khanna.
Read MoreWondering how long LASIK recovery really takes? This guide breaks down what most patients experience from the first 24 hours through the first 3 months—when vision sharpens, dryness improves, and the cornea fully stabilizes. It also covers common recovery tips, factors that can affect healing, and when to call your doctor, based on modern bladeless LASIK performed by Dr. Rajesh Khanna at Khanna Vision Institute.
Read MoreKhanna Vision Institute is expanding to bring more patients access to advanced vision correction, modern diagnostics, and a smoother, more personalized care experience. This update highlights new investments in imaging and laser technology, improved surgical facilities, enhanced patient education resources, and greater availability of procedures like SMILE, LASIK, EVO ICL, PIE, and advanced cataract surgery—all led by Dr. Rajesh Khanna.
Read MoreKeratoconus is a progressive condition that thins and reshapes the cornea, causing blurred, distorted, and constantly changing vision. This guide explains common symptoms, risk factors, and how advanced diagnostics like corneal mapping help detect keratoconus early. It also outlines today’s proven treatment options—custom contact lenses, corneal cross-linking (CXL), CTAK, topography-guided PRK with cross-linking, and corneal transplant—offered by Dr. Rajesh Khanna at Khanna Vision Institute.
Read MoreChoosing the right vision procedure after 40 depends on more than your prescription. This article compares PRK (corneal laser reshaping) with PIE (Presbyopic Implant in Eye), a lens-based solution designed to restore near and distance vision while reducing reliance on reading glasses. Learn the key differences in how each procedure works, recovery expectations, ideal candidates, and why PIE may be a longer-lasting, age-proof option for presbyopia at Khanna Vision Institute with Dr. Rajesh Khanna.
Read More
Celebrate Independence Day with the freedom of clear vision. This limited-time LASIK special explains how modern, blade-free, all-laser LASIK can reduce or eliminate dependence on glasses and contact lenses with a fast procedure and quick recovery. Learn about benefits, safety technology, who qualifies, and how a personalized evaluation at Khanna Vision Institute with Dr. Rajesh Khanna can help you choose the best option—LASIK, SMILE, or EVO ICL.
Read More
Turn back the clock on aging vision with PIE (Presbyopic Implant in Eye)—a modern lens-replacement procedure designed to restore clear sight at near, intermediate, and distance ranges. In about 7 minutes per eye, PIE replaces the stiff, aging natural lens with a premium intraocular lens (IOL), helping many patients reduce or eliminate dependence on reading glasses while also preventing future cataracts. Learn how PIE compares to LASIK/SMILE, what to expect during recovery, and which advanced lens options may fit your lifestyle at Khanna Vision Institute with Dr. Rajesh Khanna.
Read MoreClear vision can make a real difference on the golf course—especially when presbyopia starts affecting near focus, depth perception, and ball tracking. This article explains how Presbyopic Implant in Eye (PIE) surgery can restore near, intermediate, and distance clarity with advanced lens options, helping golfers and active adults reduce dependence on glasses and enjoy sharper, more confident vision.
Read MoreA patient’s words—“I wish I could see my mother’s face”—show how vision loss can affect emotion and connection. This guide explains common causes and today’s solutions, from cataract surgery and advanced lens implants to LASIK, SMILE, and EVO ICL at Khanna Vision Institute with Dr. Rajesh Khanna.
Read MoreiStent Glaucoma Procedure | Khanna Vision Institute (function () { "use strict"; var CFG = { baseUrl: "https://khannainstitute....
Read MoreSMILE Vision Correction for Beach Lifestyles | Khanna Vision Institute (function () { "use strict"; var CFG = { baseUrl: "https...
Read MoreSMILE Eye Surgery Recovery | Khanna Vision Institute (function () { "use strict"; var CFG = { baseUrl: "https://khannainstitute...
Read MoreUse Your Tax Refund for LASIK | Khanna Vision Institute (function () { "use strict"; var CFG = { baseUrl: "https://khannains...
Read MoreSMILE Eye Surgery in Los Angeles | Khanna Vision Institute (function () { "use strict"; var CFG = { baseUrl: "https://khannains...
Read MoreMyopia, Hyperopia, and Astigmatism | Khanna Vision Institute (function () { "use strict"; var CFG = { baseUrl: "https://khannai...
Read More
Discover how upper blepharoplasty can restore youthful, natural-looking eyelids and improve vision. Learn about the procedure, recovery, and benefits from Dr. Rajesh Khanna.
Read MoreUnderstanding SMILE Eye Surgery (function () { "use strict"; var CFG = { baseUrl: "https://khannainstitute.com", orgName: "...
Read MoreGlaucoma Surgery for Aging Eyes | Khanna Vision Institute (function () { "use strict"; var CFG = { baseUrl: "https://khannainst...
Read MoreEye Allergies Explained | Causes, Symptoms, and Treatment (function () { "use strict"; var CFG = { baseUrl: "https://khannains...
Read MoreSMILE Laser Eye Surgery Results (function () { "use strict"; var CFG = { baseUrl: "https://khannainstitute.com", orgName: "...
Read MoreWhy Patients Trust Khanna Vision Institute for Advanced Eye Care (function () { "use strict"; var CFG = { baseUrl: "https://kha...
Read MoreHow can presbyopic implants help you see clearly at every distance—without glasses? If reading screens is getting harder, night driving feels stressful, or astigmatism makes vision inconsistent, you’re not alone—especially after 40. For people who work under pressure (like a fire captain), glasses can fog, slip, and slow you down. Tecnis toric multifocal presbyopic implants can correct presbyopia + astigmatism + distance vision in one long-term solution—often reducing (or eliminating) dependence on glasses for daily tasks. At Khanna Vision Institute, Dr. Rajesh Khanna performs a detailed evaluation (eye health, corneal shape, lifestyle needs) to confirm if you’re a good candidate and which lens option is safest. If you want clearer near + distance vision and a more “maintenance-free” life, book a consultation and get a personalized plan.
Read More
How can upper eyelid surgery improve your vision? If your upper lids feel heavy—or your “hooded” skin blocks your side or upper view—daily tasks like driving, reading, and screens can become tiring. Upper blepharoplasty isn’t only cosmetic; for many patients it restores a clearer field of vision by removing excess skin (and, when needed, tightening support tissue) so the eyes open naturally again. At Khanna Vision Institute, Dr. Rajesh Khanna evaluates whether your droopy lids are truly affecting vision—often using visual field testing—then recommends the safest, most natural plan. If your eyelids are blocking vision, the procedure may be considered functional (not just cosmetic), which can sometimes support insurance approval. Book a consultation and get clarity on what’s causing the heaviness—and what your best option is.
Read MoreHow much is LASIK with insurance? Most plans label LASIK as “elective,” so they don’t pay the full cost—but many patients still save with employer vision discounts and smart payment options. If you’re tired of spending year after year on glasses, contacts, solutions, and replacements, LASIK can feel like a one-time upgrade that pays you back over time. At Khanna Vision Institute, Dr. Rajesh Khanna explains pricing clearly, checks whether your plan offers LASIK discounts, and shows how FSA/HSA (pre-tax) savings and 0% financing (for qualified patients) can make treatment realistic. If LASIK isn’t the best fit, you’ll also learn about SMILE, EVO ICL, and PIE—so you choose the safest option, not just the most popular one. Book a consultation and get an honest plan in minutes.
Read MoreLASIK for Reading (Monovision LASIK) can reduce or eliminate reading glasses after 40. If menus, phone text, and screens are getting harder to focus on, that’s usually presbyopia—an age-related near-vision change almost everyone experiences. Readers help, but they’re annoying to carry, switch, and lose. Monovision LASIK is customized so one eye is optimized for distance and the other for near, and your brain blends the two for everyday tasks—reading, driving, and computer use. At Khanna Vision Institute, Dr. Rajesh Khanna maps your eyes and explains whether Monovision LASIK, PIE (presbyopic implants), or another option fits your goals—clearly and honestly. If you want freedom from “readers,” book a consultation.
Read MoreHELLO treatment helps dry eye + recurring styes by fixing the real cause: blocked eyelid oil glands. If your eyes burn, feel gritty, get blurry on screens, or you keep getting styes again and again—drops and warm compresses often give only temporary relief. HELLO uses controlled heat + gentle pressure to clear the gland blockages, restore a healthier tear film, and reduce eyelid inflammation—with no downtime for most patients. At Khanna Vision Institute, Dr. Rajesh Khanna first checks the glands and tear film, then recommends the safest plan for long-term comfort. If you want steady relief (not just quick soothing), book a dry-eye evaluation.
Read More
Common eye surgeries for seniors can restore clear, comfortable vision—often faster than most people expect. If reading is harder, colors look dull, or lights feel more glaring, the cause may be cataracts, presbyopia, glaucoma pressure, eyelid droop, or corneal changes. At Khanna Vision Institute, we don’t “push” one procedure. We first do detailed imaging and testing, then match the right option—cataract surgery with modern IOL lenses, refractive lens exchange (RLE), glaucoma procedures (including MIGS), eyelid surgery (blepharoplasty), corneal treatments, or laser vision correction when appropriate. If you want a clear plan with honest guidance, book a consultation and get a personalized recommendation for your eyes, goals, and lifestyle.
Read MoreSMILE eye surgery for diabetic patients can be safe—when diabetes is well-controlled and the eyes are healthy. If you’re tired of glasses/contacts but worried about healing, SMILE is a minimally invasive, flap-free laser option that uses a small incision and is known for lower dry-eye risk compared with LASIK. At Khanna Vision Institute, eligibility is not “one-size-fits-all.” We first confirm stable blood sugar, check cornea + retina health, and rule out advanced diabetic retinopathy. If everything looks stable, SMILE can deliver clear, natural vision with a smooth recovery plan and close follow-up. Want the safest answer for your eyes? Book a consultation and get a personalized recommendation.
Read MoreBlade-Free Vision Correction = gentler, more precise laser treatment. If you’ve been avoiding vision correction because “surgery feels scary,” modern options are designed to be comfortable, predictable, and blade-free. At Khanna Vision Institute, your eyes are measured in detail (corneal shape, thickness, prescription stability) so the goal isn’t just clear vision—it’s the safest plan for your exact eye anatomy. Here’s the difference: SMILE is flap-free with a tiny incision and is often preferred by active patients and those concerned about dryness. Bladeless LASIK uses a femtosecond laser (no blade) for fast, crisp results. If you want freedom from glasses/contacts without guesswork, book a consultation and get a clear answer on whether SMILE or bladeless LASIK fits you best.
Read MoreFree LASIK Consultation — get clarity before you commit. If you’re tired of glasses or contact lenses, the smartest first step is a free evaluation that tells you what’s safest for your eyes—not just what’s popular. During your visit at Khanna Vision Institute, Dr. Rajesh Khanna checks corneal thickness, topography, and prescription stability, then explains whether LASIK, SMILE, or EVO ICL fits your vision goals and lifestyle. Because the real risk isn’t “choosing LASIK vs SMILE”… it’s choosing the wrong procedure without precise testing. If you want a clear answer, transparent guidance, and a plan you feel confident about—book the free consultation and get your questions answered in one visit.
Read MoreEye Dilation Exam — see what a regular exam can’t. If you’ve ever wondered why we dilate your eyes, it’s because dilation lets the doctor check the retina, macula, optic nerve, and blood vessels—the areas where serious problems can hide early. Most people worry about the blur or light sensitivity, but the bigger concern is missing an early warning sign (like diabetic eye changes, macular issues, or a retinal tear) when it’s easiest to treat. At Khanna Vision Institute, Dr. Rajesh Khanna explains each step clearly, keeps the process comfortable, and helps you plan ahead (bring sunglasses, and consider arranging a ride if you’re sensitive to light). If it’s been a while since your last dilated exam—or you have diabetes, flashes/floaters, or blurry vision—book a visit for a thorough check.
Read MoreEyeMed Vision Insurance — use your benefits to save on eye care. If you’ve been delaying an eye exam, new glasses, or contacts because of cost, EyeMed can make routine vision care much more affordable. The real risk of waiting isn’t just blurry vision—regular eye exams can catch issues early and sometimes reveal broader health red flags. At Khanna Vision Institute, our team helps you verify EyeMed benefits upfront, explain what’s covered, and estimate costs before your visit—so there are no surprises. EyeMed typically supports routine exams and can help reduce costs on eyewear and contact lenses, and many plans also include discounts for LASIK/SMILE with participating providers. If you have EyeMed and want the maximum savings + expert guidance, schedule a visit and let us walk you through your options in plain English.
Read MoreIPL for Dry Eye — lasting relief when drops don’t work. If your eyes burn, itch, feel gritty, or get worse after screens/contacts/windy air, the real problem is often blocked Meibomian glands (MGD)—your tears evaporate too fast. IPL targets the root cause (inflammation + blocked oil glands), not just symptoms. In a quick, non-invasive session (about 15–20 minutes), gentle light warms the glands to help melt hardened oils and improve tear quality—so you can feel comfortable without living on artificial tears. At Khanna Vision Institute, Dr. Rajesh Khanna confirms if IPL fits your eyes using advanced dry-eye testing, then builds a plan (often 3–4 sessions). If you want clear, calm eyes again—book a dry-eye evaluation.
Read MoreSMILE Laser Eye Surgery — flap-free clarity in 24 hours. If you’re tired of glasses/contacts (and the dryness, fogging, and daily hassle), the real need is stable, comfortable vision that fits an active lifestyle. SMILE uses a tiny 2–3 mm incision (no corneal flap), which is why many patients experience less dry eye risk and strong corneal stability—with vision often improving by the next morning. Sarah (29) came in frustrated with lenses and mild dryness. After a full evaluation, Dr. Rajesh Khanna recommended SMILE for her lifestyle. Her procedure was quick, recovery was smooth, and she was back to normal life fast—hiking, working, and living without the lens stress. At Khanna Vision Institute, your scans decide the best option (SMILE vs LASIK vs EVO ICL)—not a sales pitch. Book a consultation and get a clear, personalized plan.
Read More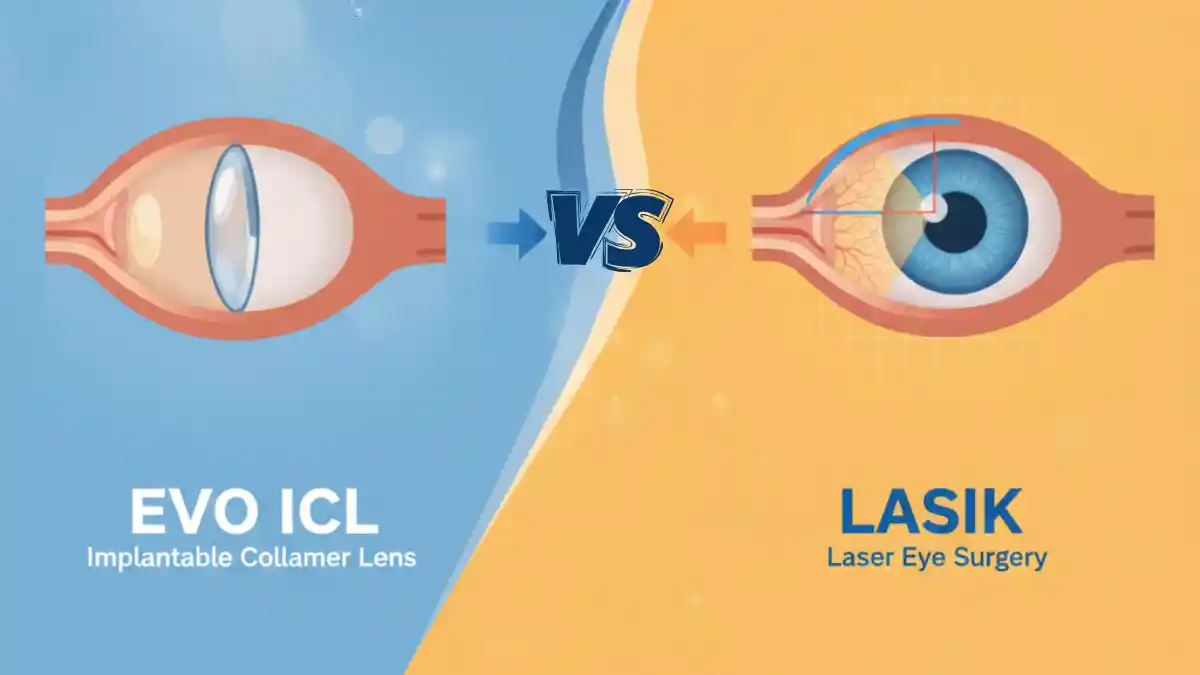
EVO ICL vs LASIK — which is safer for YOUR eyes? If you want freedom from glasses, the real question is how your eyes are built: corneal thickness, dryness, and prescription strength. LASIK reshapes the cornea and works beautifully for many people with healthy, thicker corneas and moderate prescriptions—with fast recovery and long-term results. But if you have thin/irregular corneas, higher prescriptions, or dry eye symptoms, EVO ICL can be the smarter choice because it doesn’t remove corneal tissue, often feels more comfortable for dry eyes, and is reversible if your needs change later. At Khanna Vision Institute, **Dr. Rajesh Khanna personally reviews your scans (cornea + tear film + prescription) and recommends the option that’s safest—not a one-size-fits-all sale. Book a consultation and leave with a clear plan for the procedure that fits your eyes and lifestyle.
Read MoreDoes Pterygium Need SMILE Eye Surgery? If you’re seeing a red, fleshy growth and feeling constant irritation, it’s natural to ask if SMILE can fix it. But here’s the truth: SMILE corrects prescription (myopia/astigmatism)—it does not remove pterygium tissue. If the growth is moving toward the cornea, causing blur/astigmatism, or staying inflamed, the right first step is usually pterygium excision (removal + graft to reduce recurrence). After the eye heals and the cornea stabilizes, you may still choose SMILE or LASIK to fine-tune vision—only if testing shows it’s safe for your cornea. At Khanna Vision Institute, Dr. Rajesh Khanna explains the safest sequence clearly: treat the growth first, then correct the prescription—so you get comfort, clarity, and long-term protection.
Read MoreDoes Insurance Cover LASIK? Most people assume insurance will pay—but LASIK is usually labeled “elective,” so full coverage is rare. That said, you can often lower your out-of-pocket cost through vision-plan discounts, preferred pricing, employer perks, and pre-tax FSA/HSA funds. At Khanna Vision Institute, Dr. Rajesh Khanna walks you through eligibility + payment options clearly, so you can plan with confidence—no confusion, no pressure. If you’re tired of contacts/glasses costs every year, bring your plan details to your consult and we’ll map out the best, most affordable path (LASIK, SMILE, or another option).
Read MoreIf you’re like most people, you want clear vision—but LASIK pricing can feel confusing or out of reach. This offer removes that barrier: up to 50% off LASIK without compromising safety, precision, or surgeon experience. At Khanna Vision Institute, Dr. Rajesh Khanna evaluates your eyes carefully (cornea, prescription stability, overall health) and recommends the best option—LASIK, SMILE, or another solution—based on what’s safest for you. If you’re tired of glasses, contact lens irritation, and recurring costs, this is a smart moment to book a consult and see what you qualify for.
Read MoreIf your eyes ever get red, painful, light-sensitive, or suddenly blurry while wearing contact lenses, don’t “wait it out”—a lens-related infection can worsen fast. These infections often start from simple habits like sleeping in lenses, reusing solution, or getting water in your contacts, allowing bacteria, fungi, or parasites to reach the cornea. At Khanna Vision Institute, Dr. Rajesh Khanna focuses on early diagnosis and the right drops/treatment to protect your vision—and also helps patients with recurring issues explore long-term alternatives like SMILE, LASIK, or EVO ICL to reduce contact-lens risk. If you’re having symptoms now, remove your lenses and book an evaluation.
Read MoreIf you’re suddenly holding your phone farther away or swapping reading glasses all day, presbyopia is likely the reason—and it usually starts around 40. Vuity can give a few hours of sharper near vision with daily drops, while presbyopic implants (PIE) can deliver a longer-term, glasses-reduced solution by replacing the eye’s natural lens (often ideal if cataracts are also developing). At Khanna Vision Institute, Dr. Rajesh Khanna guides you through both options in simple language, then recommends the safest match based on your exam, lens clarity, and lifestyle. If you want a plan that fits your daily work + reading needs—not a one-size-fits-all answer—book a consultation.
Read MoreIf glasses/contacts are costing you comfort, time, and money, modern LASIK can be a long-term reset—clearer vision for driving at night, sports, and everyday life. At Khanna Vision Institute, Dr. Rajesh Khanna uses advanced diagnostics and personalized measurements to confirm what’s safest for your eyes—then delivers precise laser correction with fast recovery for many patients. And if cost is the hesitation, options like financing plus FSA/HSA can make it surprisingly manageable. Want to know what you qualify for? Book a consultation.
Read MoreIf you play basketball (or even just love watching the NBA Finals), even slight blur or dry contacts can hurt timing, depth perception, and comfort. At Khanna Vision Institute, Dr. Rajesh Khanna matches you to the right option—often SMILE (flap-free) or LASIK—after a complete exam focused on safety and long-term stability. If you want clearer vision for sports and daily life, book a consultation and find out what you truly qualify for.
Read MoreWestlake Village—if glasses or irritated contacts are slowing you down, SMILE Pro is a premium, flap-free upgrade that’s minimally invasive and built for fast recovery. At Khanna Vision Institute, you get a boutique, unhurried evaluation, conservative “patient-first” guidance, and SMILE Pro on the ZEISS VisuMax 800—so you’re choosing precision, safety, and long-term stability. Want a meaningful gift or to schedule 2026 surgery? Book a consultation or call (310) 482-1240 / (805) 230-2126.
Read MoreWest Hollywood—if glasses or dry, irritated contacts are getting in the way of your lifestyle, SMILE Pro is a smarter, flap-free upgrade that’s minimally invasive and designed for fast recovery. At Khanna Vision Institute, you’ll get a boutique, unhurried evaluation, honest candidacy guidance, and advanced SMILE Pro on the ZEISS VisuMax 800—so you can feel confident you’re choosing the safest, most refined option. Want a gift that’s remembered every morning or want to schedule 2026 surgery? Book a consultation or call (310) 482-1240 / (805) 230-2126.
Read MoreThousand Oaks—if glasses or dry, irritated contacts are stealing your comfort, SMILE Pro can be the cleanest upgrade: flap-free, minimally invasive, and built for active lifestyles with fast recovery and long-term stability. At Khanna Vision Institute, you’re never rushed—just a boutique evaluation, honest candidacy guidance, and SMILE Pro on the ZEISS VisuMax 800. Want a gift that truly changes daily life or plan surgery in 2026? Book a consultation or call (310) 482-1240 / (805) 230-2126.
Read MoreSanta Monica—if glasses or irritated contacts are stealing your comfort (and you want a gift that actually changes daily life), a SMILE Pro gift certificate is a powerful upgrade. SMILE is flap-free, minimally invasive, and ideal for active lifestyles—often meaning more comfort, less dryness, and a faster return to normal routines. At Khanna Vision Institute, you’ll get a boutique, unhurried evaluation, honest candidacy guidance, and advanced SMILE Pro technology like the ZEISS VisuMax 800. Ready to gift clear vision or schedule 2026 surgery? Book a consultation or call (310) 482-1240 / (805) 230-2126.
Read MoreSan Francisco—if glasses or irritated contacts are stealing comfort (especially in the holidays), a SMILE Pro gift certificate can be a truly meaningful upgrade. SMILE is flap-free, minimally invasive, and designed for active lifestyles with fast recovery and long-term stability. At Khanna Vision Institute, you get a boutique, unhurried evaluation, honest candidacy guidance, and advanced SMILE Pro tech like the ZEISS VisuMax 800—so you know you’re choosing the safest, most refined option. Want to gift clear vision or schedule 2026 surgery? Book a consultation or call (310) 482-1240 / (805) 230-2126.
Read MoreSan Diego patients—if glasses/contacts are ruining comfort and you want the most advanced, minimally invasive option, SMILE Pro can be a life-changing upgrade. It’s flap-free, uses a tiny incision, and is built for active lifestyles with fast recovery and strong long-term stability. At Khanna Vision Institute, you’ll get a boutique, unhurried evaluation, honest candidacy guidance, and SMILE Pro on the ZEISS VisuMax 800. Want to gift clear vision or schedule 2026 surgery? Book a consultation or call (310) 482-1240 / (805) 230-2126.
Read MoreWhy Choose Khanna Vision Institute for SMILE Surgery (function () { "use strict"; var CFG = { baseUrl: "https://khannainstitute...
Read MoreUpper Eyelid Surgery (Blepharoplasty) | Khanna Vision Institute (function () { "use strict"; var CFG = { baseUrl: "https://khan...
Read MoreTissue-Addition Keratoplasty (CTAK) is an advanced option for selected keratoconus patients in Los Angeles who need more than glasses or contact lenses. Khanna Vision Institute explains how CTAK works, who it may help, recovery, risks, alternatives, costs, locations, and includes a CTAK surgery video for clearer decision-making.
Read MoreSMILE Eye Surgery – A Gentle Alternative to Glasses and Contacts (function () { "use strict"; var CFG = { baseUrl: "https://kha...
Read MoreLaser Eye Surgery for Basketball Players | Khanna Vision Institute (function () { "use strict"; var CFG = { baseUrl: "https://k...
Read More
Discover SMILE, the latest FDA-approved vision correction procedure. Learn how this advanced laser eye surgery offers clear, comfortable vision with minimal downtime and excellent results.
Read MoreSMILE Eye Surgery | The Future of Vision Correction in Los Angeles (function () { "use strict"; var CFG = { baseUrl: "https://k...
Read More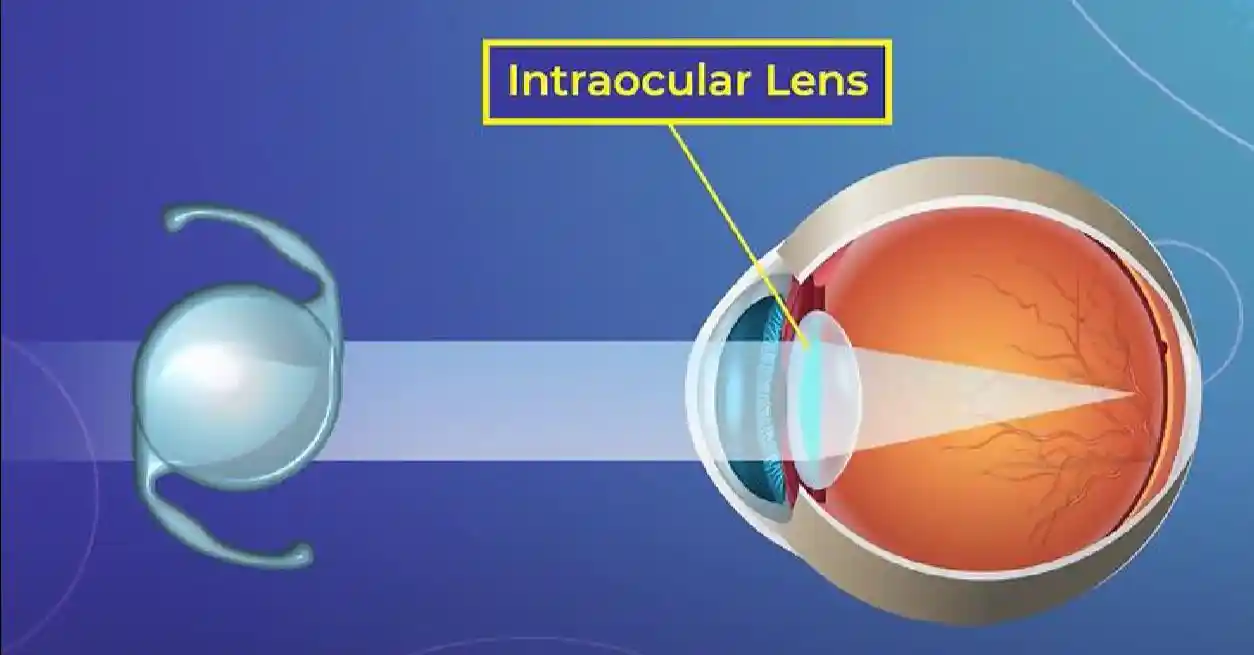
Explore the IC-8 Small Aperture Intraocular Lens — a breakthrough technology that provides clear vision at all distances. Learn about its evolution, benefits, and how it can transform your vision.
Read More
Discover if you're an ideal candidate for SMILE eye surgery. Learn about candidacy requirements, benefits, and how this flap-free procedure can transform your vision and lifestyle.
Read MoreA gift of SMILE Laser eye surgery at Thanksgiving
Read More
Discover why clinical studies show LASIK offers better vision, comfort, and long-term satisfaction than contact lenses. Learn about the benefits of permanent vision correction.
Read More
Discover SMILE, the advanced flap-free laser vision correction procedure. Learn how this gentle, minimally invasive surgery can help you see the world with clarity, comfort, and confidence.
Read More
Learn about SMILE laser eye surgery, a modern, minimally invasive alternative to LASIK. Discover how this flap-free procedure offers faster healing and greater comfort for vision correction.
Read More
Discover the field of ophthalmology and how it helps diagnose and treat eye conditions. Learn about common eye diseases, advanced diagnostics, and expert care from Dr. Rajesh Khanna.
Read More
Explore the six leading advantages of LASIK eye surgery, from fast recovery to long-lasting results. Learn why millions trust this procedure for clear, natural vision.
Read More
Discover if LASIK is the right solution for your nearsightedness. Learn about the procedure, candidacy requirements, effectiveness, and safety from Khanna Vision Institute.
Read More
Master the proper technique for applying eye drops and ointments. Learn step-by-step instructions, hygiene tips, and common mistakes to avoid for effective eye care.
Read MoreGive a premium Christmas vision gift for Orange County. An EVO ICL gift certificate helps your loved one reduce dependence on glasses or contacts and move toward clear, crisp vision with expert care at Khanna Vision Institute. Purchase now and schedule evaluation or surgery in 2026—ideal for using 2025 FSA/HSA benefits before December 31. Gift certificates never expire, are transferable, and can be applied toward EVO ICL or other vision correction options.
Read MoreCataract surgery for older adults replaces the cloudy natural lens with a clear IOL to restore brighter, sharper vision. It’s quick, usually painless with numbing drops, and most patients see improvement within a day or two.
Read MoreSMILE Vision Correction (function () { "use strict"; var CFG = { baseUrl: "https://khannainstitute.com", orgName: "Khanna...
Read More
Learn how LASIK eye surgery can transform your snowboarding experience. Discover the advantages of clear, fog-free vision on the slopes and why athletes trust Dr. Rajesh Khanna.
Read MoreTired of squinting at your phone or juggling reading glasses? Discover the revolutionary new Vizz™ presbyopia eye drops and PIE (Presbyopic Implant in Eye) surgery by world-renowned eye surgeon Dr. Rajesh Khanna. Serving Beverly Hills and Westlake Village, Khanna Vision Institute delivers the most advanced, personalized solutions for age-related vision loss — helping you see clearly at all distances and live life glasses-free. Find out which treatment is right for you and take the first step toward visual freedom today.
Read More
Discover how LASIK and advanced vision correction techniques can help treat presbyopia. Learn about Presby-LASIK, PIE, IC-8 IOL, and other modern solutions from Khanna Vision Institute.
Read More
Learn about breakthrough treatments for adult amblyopia (lazy eye). Discover how modern vision therapy and advanced technology can help adults improve their vision and quality of life.
Read More
Learn about three innovative eye surgeries that can permanently correct astigmatism: LASIK, SMILE, and Toric IOL implants. Discover which procedure is right for you.
Read MoreBest SMILE Surgeon in Los Angeles /* ===== Scoped SMILE Expert Content Styling ===== */ .smile-expert-wrapper { max-wid...
Read More